Send Feedback
Print
Mobile
Back
Myocardial Infarction
Definition
The diagnostic criteria for acute myocardial infarction are elevated biochemical markers of myocardial necrosis (e.g., troponins) associated with at least one of the following:
- Ischaemic symptoms
- New Q waves on ECG
- ST segment or T wave changes on serial ECGs.
Causes
Acute coronary occlusion due to:
- Coronary artery plaque rupture and thrombosis.
- Spontaneous coronary dissection (rare; occurs mainly in young women).
- Emboli (rare).
Note: Other cardiac conditions such as myocarditis and stress cardiomyopathy (Takotsubo cardiomyopathy) may mimic myocardial infarction.
Note: Troponins may be elevated in other conditions. See Troponin Testing.
Clinical features
A history of severe crushing retrosternal chest pain radiating to neck and arms is typical. However, atypical presentations are very common. May present as collapse, LVF, hypotension, peripheral embolus, stroke, or "malaise". A difficult diagnosis to exclude even with normal ECG. Generally if in doubt, admit to hospital. Patients with chest pain of low probability for coronary cause and other major pathology excluded, should be admitted to the Chest Pain Unit for exclusion of myocardial infarction. If the initial ECG is normal then the diagnosis may be suspected on the basis of history alone and ECG repeated in 2-4 hours. If ST segment depression is present, or ST-T wave changes are non-specific, but risk factors/symptoms suggest myocardial infarction, give beta-blockers, aspirin, and nitrates. See below.
Investigations
- The initial ECG on presentation determines the management strategy:
- If it shows ST elevation, the patient should be considered for immediate reperfusion (discuss with Cardiologist). Often no further tests are required prior to instigating treatment.
- Otherwise, the diagnosis will rest on serial ECGs and myocardial injury markers.
- Serial ECGs on 3 occasions 6 hours apart and before discharge. Repeat ECG when pain resolved or if pain recurs. Consider performing right sided leads for ST elevation, i.e., look actively for right ventricular infarction. May be useful in inferior infarction with heart block.
- Cardiac Injury Markers: A troponin and creatine kinase (CK) should be done on admission and at 8 to 12 hours.
- CXR can usually wait until normal working hours or prior to discharge. Indications for urgent X‑ray include moderate or severe cardiac failure.
- CBC + diff.
- Na, K, creatinine, glucose.
- Total fasting cholesterol, HDL cholesterol and triglycerides on admission and repeat at 3 months.
- Patients with suspected myocardial infarction require rhythm monitoring (CCU or telemetry).
- If suspicion of aortic dissection, arrange an urgent CT scan and inform the Cardio-Thoracic team - see Thoracic Aortic Dissection.
Management of ST Elevation Myocardial Infarction (STEMI)
- All patients presenting with acute myocardial ischaemic symptoms lasting more than 30 minutes with ST elevation on ECG.
- New ST elevation greater than 1 mm in at least 2 limb leads or greater than 2 mm in at least 2 pre-cordial leads or new left bundle branch block with typical symptoms.
- Acute reperfusion therapy is beneficial if the duration from onset is <12 hours and occasionally up to 24 hours from onset of symptoms particularly if pain is ongoing or marked ST elevation present.
- Remember "time is muscle" - expedite treatment and assess suitability for reperfusion by angioplasty urgently (thrombolysis is rarely given if angioplasty is available).
- Contact Catheter Laboratory and transfer patient - any patient with acute myocardial infarction is at risk of an acute arrhythmia and should be discussed with the Consultant. Normally a patient can remain in ED but if there are going to be delays the patient should transfer to CCU and thrombolysis should be considered.
- Stable patients with suspected myocardial infarction require a telemetry bed or admission to CCU. For advice on admission contact the Cardiology Registrar on call.
- IV access - IV insertion on admission. Flush 4-6 hourly with sodium chloride 0.9%.
- Pain relief - continuing pain suggests ongoing ischaemia which should be treated with nitrates, beta-blockers, calcium antagonists and morphine as required. Give morphine IV according to severity and repeat up to 4 hourly if necessary. Draw morphine 10 mg (1 mL) up with 9 mL of water for injection (1 mg/mL). Give 2-3 mg (2-3 mL) increments until pain is controlled observing the patient's BP and respiration. Metoclopramide 10 mg IV may reduce nausea and vomiting.
- Antiplatelet therapy:
- Give aspirin to all patients, 300 mg chew and swallow stat, then 150 mg daily. If ticagrelor is also to be given, the dose of aspirin should not exceed 100 mg daily.
- If the patient is scheduled for angioplasty, give ticagrelor 180 mg PO stat, then 90 mg BD PO unless the patient is deemed a high bleeding risk (CrCl <30 mL/min or severe liver impairment).
- If the patient is scheduled to receive thrombolysis, or is deemed a high bleeding risk, give clopidogrel 600 mg PO stat then 75 mg daily provided the patient is under 75. If over 75, give clopidogrel 300 mg PO stat, then 75 mg PO daily.
- Oxygen - should only be administered if the sat.O2 <92%.
- Nitrates may be helpful for continuing pain (patch or isosorbide mononitrate tablets). IV infusion may be preferred to oral nitrates if the patient has unremitting angina, is haemodynamically unstable and to help reduce preload in pulmonary oedema. Nitrates should be given in ICU/CCU. Remember that IV infusion for more than 24 hours may result in nitrate tolerance. Start other anti-anginals during the first 24 hours of nitrate infusion. Use glyceryl trinitrate 50 mg in 250 mL 5% glucose in a non-PVC bag (200 microgram/mL). Start infusion at 10 microgram per minute (3 mL/h). Increase infusion rate by 10 microgram/minute every 3 to 5 minutes. Boluses of 10 - 20 microgram can be given until pain relieved or BP falls (can go as low as 90 mm Hg systolic if otherwise well).
Current Indications for Thrombolysis
- Where angioplasty is not available.
- If there is a delay in access to catheter laboratory, it can be considered (e.g., if both labs are occupied or if the patient has been assessed in a rural setting >45 minutes from hospital). An r-tPA (e.g., tenecteplase) is recommended.
- A combined approach, thrombolysis and angioplasty, may be appropriate when access to the catheter lab is delayed (>60 minutes). In this situation half dose tenecteplase is administered along with IV unfractionated heparin. Give an IV bolus of unfractionated heparin of 80 units/kg with a maximum dose of 10,000 units. The patient can then be transferred to the catheter laboratory when this is available.
Thrombolytic Therapy
The Christchurch Cardiology department runs a 24 hour service for ST elevation myocardial infarction.
The current favoured thrombolytic agent is tenecteplase.
Thrombolysis Therapy
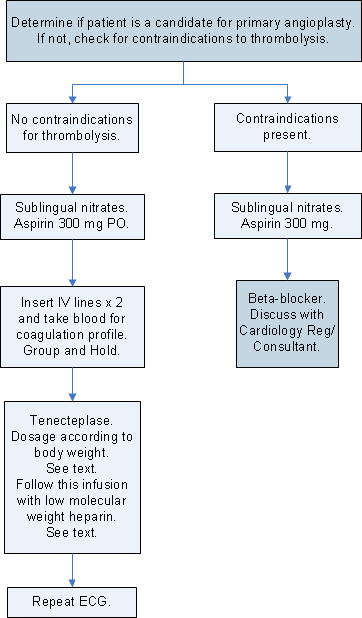
Contraindications to Thrombolysis
Absolute Contraindications:
- Any prior intracranial haemorrhage.
- Known structural cerebral vascular lesion.
- Known malignant intracranial or spinal neoplasm or arteriovenous malformation.
- Ischaemic stroke within 3 months, except if ischaemic stroke is being treated by thrombolysis.
- Neurosurgery within 6 months.
- Suspected aortic dissection.
- Active bleeding or bleeding diathesis (excluding menses).
- Significant closed-head or facial trauma within 3 months.
- Uncontrolled hypertension on presentation (SBP >180 mm Hg or DBP >110 mm Hg).
- Recent internal bleeding within 6 weeks.
- Major surgery or major trauma <2 weeks.
Relative Contraindications (to be discussed with Physician):
- Transient ischaemic attack <6 months.
- Traumatic cardiopulmonary resuscitation <2 weeks.
- Non-compressible vascular puncture.
- Pregnancy.
- Active peptic ulcer.
- Current use of anticoagulants (e.g., warfarin with an INR >2: the higher the INR, the higher the risk of bleeding).
Administration of Tenecteplase
- Give single bolus IV, dosage according to weight:
Weight
|
Dose of Tenecteplase
|
<60 kg
|
30 mg
|
60 - 70 kg
|
35 mg
|
70 - 80 kg
|
40 mg
|
80 - 90 kg
|
45 mg
|
>90 kg
|
50 mg
|
Administration of Heparin in association with Tenecteplase
Enoxoparin 1 mg/kg subcut q12h for 48 hours post thrombolysis. Give first dose after completion of tenecteplase if no abnormal bleeding has occurred.
Note: Failed thrombolysis may be an indication for emergency angiography/angioplasty.
Further Guidelines on Management of STEMI
- Continue antiplatelet drugs as appropriate.
- If the patient has had an angioplasty, do not give heparin. Where thrombolysis is contraindicated and angioplasty is not done, give a low molecular weight heparin, e.g., enoxaparin 1 mg/kg subcut q12h. The usual duration of enoxaparin treatment is 48 hours. The dosage of LMWH will need to be reduced if there is significant renal impairment (CrCl <60 mL/min) or for extremes of weight. See the VTE section.
- Anti-Xa monitoring is recommended if the duration of LMWH therapy is >48 hours. Treatment for longer than 48 hours is associated with an increased risk of haemorrhagic complications and would normally only be considered in patients with ongoing unstable ischaemic symptoms, following discussion with the Consultant, and with intensified monitoring for haemorrhagic complications.
- If there is severe renal impairment or if reversal of the heparin effect is likely to be needed, consider a continuous infusion of unfractionated heparin and monitor the APTT (see Unfractionated Heparin Dosage). The APTT "therapeutic range" will vary according to the test used in the laboratory. Contact the laboratory for their recommended therapeutic range.
- Hypnotics if sleep disturbed.
- Beta-blockers - continue if patient is already on them and no contraindication exists. Beta-blockers improve medium term prognosis, and unless contraindications are present, beta-blockers such as atenolol (25-50 mg PO daily) or metoprolol (23.75 - 95 mg PO daily), should be commenced on admission, and given IV if continuing pain/arrhythmias. Dosages should be increased as tolerated during admission. They should be continued for at least 2 years. Avoid in the first few hours after an inferior MI unless sinus tachycardia present.
- Amiodarone may be indicated for some atrial and ventricular arrhythmias. Discuss with Cardiologist.
- Continuing chest pain in spite of appropriate morphine IV and sublingual nitrates. Consider beta-blocker therapy but remember that patients may benefit from early intervention. Nitrate infusion may also be helpful.
Troponin Testing
- Cardiac troponins are highly cardiac specific. High-sensitivity troponin I is the troponin test currently available at Canterbury Health Laboratories.
- No circulating troponin should be present in the serum of a healthy individual.
- Troponins rise in the circulation 2-6 hours after myocardial injury, therefore troponins may be undetectable in blood taken from patients with acute myocardial infarction at the time of presentation to hospital. It is recommended that an initial negative sample be repeated once after 8 - 12 hours.
- Troponins remain elevated for up to 14 days after acute myocardial infarction.
- Other biochemical markers, such as myoglobin or CK must be used during this period if further acute myocardial infarction is suspected.
- Once a biochemical diagnosis of myocardial infarction has been made there is little clinical utility in repeat testing.
- If a patient presents with a suspected MI and renal failure, an elevated troponin level needs to be interpreted with caution. Troponin levels may be elevated in renal failure.
- Not all myocardial injury is caused by coronary occlusion. Elevations in troponin may also be seen in myocarditis, direct cardiac trauma, heart failure, and pulmonary embolism.
- Small rises in troponin are commonly seen following major surgery and major medical illness especially in the elderly. Whilst this almost certainly reflects myocardial necrosis, the clinical implications of troponin elevations in these patients have not been defined. It is probable these patients will have underlying coronary disease and secondary prevention strategies for coronary disease should be considered (aspirin, statin, beta-blocker).
In-Hospital Management following Myocardial Infarction
- Mobilization protocols - these protocols are available in CCU and Cardiology Ward. Some patients can be discharged as early as three days after admission.
- Investigation after myocardial infarction:
- Echocardiography should be considered in all patients to assess left ventricular function for prognostic reasons and review the need for on-going therapy with ACE inhibitors.
- Coronary angiography should be considered in all patients, including non-ST elevation MI and post infarction angina.
- Medical therapy should be tailored to each individual patient, but should include aspirin and clopidogrel (or ticagrelor) unless contraindicated (see Management of ST Elevation Myocardial Infarction for dosage recommendations). Beta-blockers should also be given unless contraindicated, and ACE inhibitors given if there is evidence of left ventricular dysfunction. Statins should be considered in all patients unless contraindicated. Nitrates are appropriate for control of symptoms. There is little evidence that calcium antagonists improve prognosis following myocardial infarction. However, the use of diltiazem or verapamil could be considered in patients who have contraindications to beta-blocker therapy and have good left ventricular function without clinical evidence of congestive failure.
- Aim to reduce the effects of any risk factor present - smoking cessation, cholesterol lowering agents, control of hypertension, diet if overweight.
- Ask for Cardiac Rehabilitation Nurse (pager 8262) to review prior to discharge.
Reference: ST-elevation myocardial infarction: New Zealand management guidelines. Cardiac Society of Australia and New Zealand. NZMJ 118 7 Oct 2005.
Complications of Myocardial Infarction
The following problems may complicate even small myocardial infarcts:
- Left ventricular failure.
- DVT/PE.
- Dressler's syndrome (pericardial and/or pleural inflammation).
- Arrhythmias.
- Cardiogenic shock/low cardiac output states.
- Valvular dysfunction.
- Myocardial rupture (septal or free wall).
- Mural thrombi (with systemic embolization).
Topic Code: 2206