Send Feedback
Print
Mobile
Back
Thoracic Aortic Dissection
Clinical Features
This diagnosis should be considered in all patients presenting with chest pain. There are no specific clinical features, and therefore a high index of suspicion is necessary as this diagnosis is often missed. Patients nearly always present with severe knife-like pain often described as stabbing.
Once the index of suspicion is raised, it is to be treated as though it is a type A dissection until proven otherwise. This is because the mortality for a type A dissection is approximately 2%/hour.
Type A dissection involves the ascending aorta, and in type B dissection the ascending aorta is not involved.
Aetiology
Cystic medial necrosis; Marfan's syndrome; atherosclerosis; hypertension; trauma; post-cardiac surgery; pregnancy.
Investigations
See Diagnosis of Aortic Dissection.
There are only two useful investigations on which decisions should be made. They are CT scan with contrast or a trans-oesophageal echo. The preference at Christchurch Hospital is to perform a CT scan. Delaying a diagnosis to obtain a chest X-ray etc. is dangerous and inappropriate.
Diagnosis of Aortic Dissection
Diagnosis of Aortic Dissection
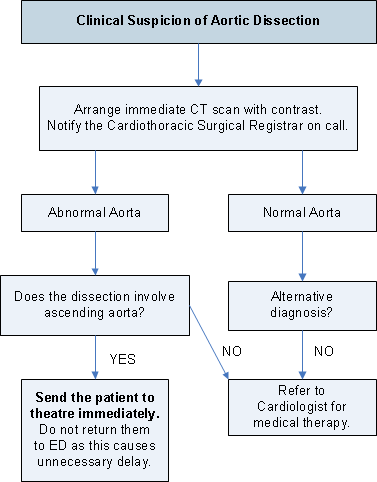
Note: The CT suite needs to be contacted and advised to stop scanning other patients with this patient taking priority.
Treatment - Type A
- Utilize time while waiting for transport to CT scanner. Contact the Cardiothoracic Surgical Registrar on call. Place urinary catheter, give adequate analgesia, e.g., IV morphine. Initiate infusion of hypotensive drugs. See below. Draw bloods for cross-match, CBC, Na, K, creatinine. Cross-match six units. An ECG should also be done.
- Medical management: Until the patient is placed on by-pass, aggressive medical management should be pursued immediately. This will be guided by the Cardiothoracic Surgical Registrar, who will also ensure that the operating theatre is kept fully informed. The principle is to lower the blood pressure and the force of contraction. This is best done with vasodilators and concurrently with negative inotropes. Do not use vasodilatation on its own as this will only increase cardiac output and stress the false lumen.
- Start a labetalol infusion. Give intravenous and later oral beta-blockers, e.g., labetalol, unless contraindicated (systolic BP <120, cardiac failure, bradycardia <60/minute, heart block, obstructive airways disease) and start a glyceryl trinitrate infusion or a sodium nitroprusside infusion. Aim to reduce the systolic blood pressure to between 100 and 120 mm/Hg to reduce the contractility of the left ventricle. Monitor blood pressure and urine output. Consider prochlorperazine to reduce the risk of vomiting.
- The patient must be accompanied to the CT suite by both doctor and nurse so that medical management, i.e., blood pressure control is applied aggressively and continued until the patient is in theatre and placed on by-pass.
- The aim is to have a patient in the operating theatre within half an hour of a clinician raising the question "is this an aortic dissection?"
Treatment - Type B
- Refer to Cardiologist and Consultant Vascular Surgeon. These patients are generally managed by vascular surgery but may occasionally be admitted to CCU for control of labile hypertension. Aim to keep systolic BP 100-120 mm Hg. The first line drug to use is labetalol by IV infusion, then oral with other anti-hypertensive drugs as required.
- Morphine for pain with antiemetics.
- Patients should be monitored for complications of dissection. These include mesenteric, renal, or lower limb ischaemia. Consult the Vascular Surgeon if any of these complications occur.
Topic Code: 1343