CDHB
This is established by the Dix Hallpike test.
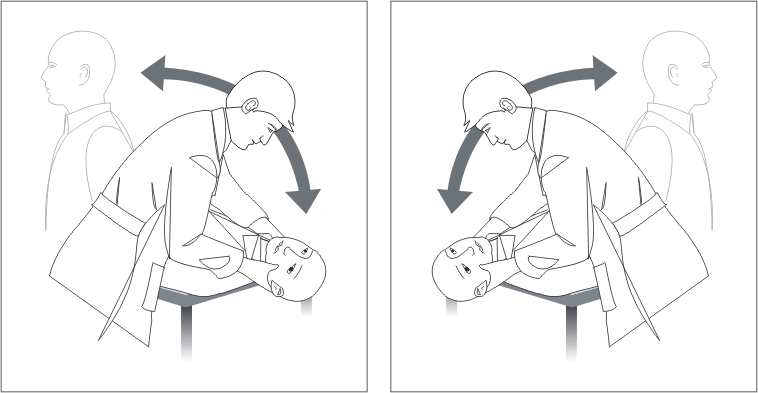
The patient sits with legs extended near the end of the examination table. The examiner turns the head 45 degrees to one side and lies the patient down so the head is below the table. For a positive test the patient must experience acute vertigo and have brisk torsional nystagmus which is anticlockwise to the right ear or clockwise to the left ear.
The test requires some experience to perform well and safely. Seek advice from a more senior colleague if you are unsure.
The Epley Canalith Repositioning Procedure (CRP) can be performed once a certain diagnosis of BPV has been made. Once again, this procedure requires experience. Seek advice.
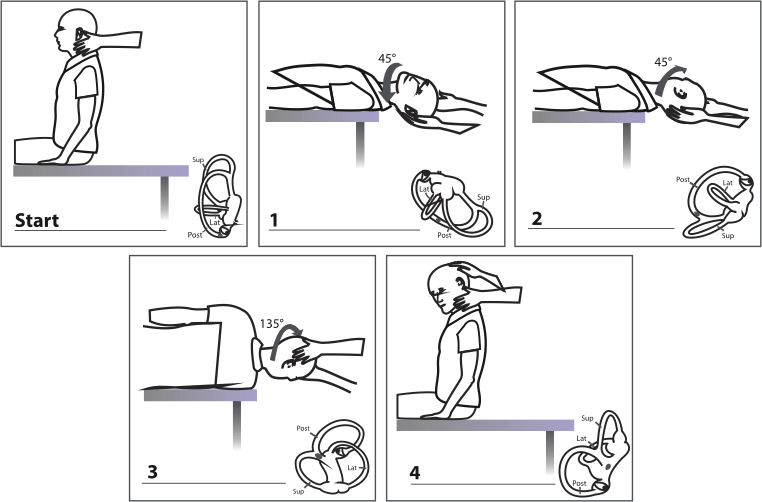
The repositioning procedure is designed to remove the particle(s) from the posterior semicircular canal. The drawings illustrate treatment for the left ear. The physician stands or sits behind the patient at the head of the table. From the start position the head is turned 45 degrees and the patient tipped back (1) (identical to the Dix-Hallpike test). Wait for the nystagmus to cease, then turn the head 45 degrees to the other side (2). Wait. Ask the patient to turn the body and head to 135 degrees (looking down at the floor) (3). Wait. Ask the patient to straighten up and sit up with the head tilted to the treated side (4). Repeat the Dix-Hallpike test. If no response, cease. If positive, repeat the Epley Canalith Repositioning Procedure once.
Special care is required for patients with back and neck problems.
Acute vertigo is the only symptom, due to sudden unilateral vestibular failure (probably viral) of the superior and/or inferior vestibular nerve. The nystagmus is always unidirectional and rotatory-horizontal with the fast phase away from the affected side. The patient is usually able to stand but prefers to lie. The head impulse test (see below) is abnormal on the affected side. The acute vertigo can last up to a week. Balance recovery can take a month, and longer in older individuals. Benign positional vertigo can follow. The main differential diagnosis is cerebellar infarction.
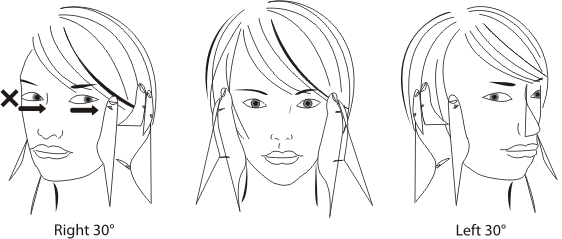
This is to test the normality or absence of the vestibulo-ocular reflex (VOR). The patient should be sitting upright staring at the examiner's nose. The examiner turns the head from the midline sharply to one side 30 degrees. The test is positive if the eyes make saccades to refix on the nose target. In the illustration the test to the left is normal (eyes fixed on target). Thrust of the head to the right results in corrective saccades to the left, indicating a right VOR abnormality.
Inner ear disorder with attacks of vertigo (<12 hours) usually accompanied by deafness, tinnitus and aural fullness (blocked feeling) in the affected ear. Nystagmus is rotatory-horizontal, often initially towards the symptomatic ear and later away from it. Occurs in middle-aged and older adults. Diagnosis is established by electrocochleography.
Topic Code: 3773