Send Feedback
Print
Mobile
Back
Paracetamol
- 140 mg/kg is the threshold dose at which an oral overdose can cause hepatotoxicity in adults. Hepatotoxicity is not uncommon but fatalities are rare. Charcoal may be useful up to 2 hours.
Follow the MJA paracetamol poisoning guideline unless there are good reasons for deviating (Chiew AL, Fountain JS, Graudins A, et al. Summary statement. New guidelines for the management of paracetamol poisoning in Australia and New Zealand. Med J Aust 2015; 203: 215-218. doi: 10.5694/mja15.00614).
- Single dose, staggered dose and late presentations of paracetamol poisoning are described and management guidelines provided. Access at TOXINZ.com or from ED.
- Blood levels direct treatment. In adults, levels should be taken at 4 hours (or immediately if presentation is more than 4 hours after the ingestion). Use the green lithium heparin tube.
- Treatment is effective if begun within 8 hours. Therefore the N-acetylcysteine infusion may await the result of the 4 hour blood test. Those with massive ingestion presenting after 8 hours, especially if symptomatic, should have N-acetylcysteine without waiting for the blood level result.
- Clinical toxicity follows four approximate stages:
- 1/2 - 24 hours: nausea, vomiting, malaise (or asymptomatic).
- 24 - 48 hours: right upper quadrant pain and raised transaminases. May be oliguric if dehydrated or has developed renal toxicity.
- 72 - 96 hours: peak of transaminase elevation, bilirubin and prothrombin time. Nausea and vomiting returns. Elevated creatinine. Fetal death if pregnant.
- 4 days to 2 weeks: resolution or hepatic failure (then either transplant or death).
Note: Treatment is directed by the nomogram.
Note: Treat all patients with plasma levels above the nomogram line with N-acetylcysteine.
Note: Ensure that the correct units are used (i.e. micromol/L or mg/L) when plotting on the nomogram.
Paracetamol Toxicity Treatment Nomogram
Paracetamol Toxicity Treatment Nomogram
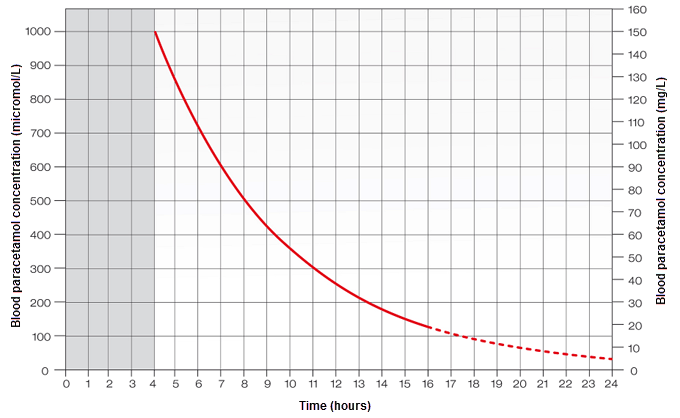
Reference: Daly FF, Fountain JS, et al. Med J Aust 2008; 188: 296-301. Adapted from Smilkstein MJ et al. Ann Emerg Med 1991; 20: 1058-63.
N-acetylcysteine Dosage in Paracetamol Poisoning
|
N-acetylcysteine:
INITIALLY: 150 mg/kg in 200 mL 5% glucose over 60 minutes
THEN: 50 mg/kg in 500 mL 5% glucose over 4 hours
THEN: 100 mg/kg in 1000 mL 5% glucose over 16 hours
|
- Calculate the dose using the patient’s actual weight, to a ceiling of 110 kg.
- N-acetylcysteine is most effective when given within 15 hours of ingestion but there is some evidence that even beyond 24 hours, it may be beneficial.
- N-acetylcysteine given after 10-14 hours post ingestion assists in the repair of hepatic damage rather than providing an alternative source of sulphydryl groups as a protective substance. This will be independent of plasma paracetamol concentration making such measurements valueless in this regard. Therefore late paracetamol levels (>15 hours) will not be a useful guide to treatment, and levels beyond 24 hours are pointless. Instead be guided by tests of liver function as described above.
- Anaphylactoid reactions:
- If rash or urticaria develop during the N-acetylcysteine infusion, slow or stop the infusion, treat with promethazine 25 mg IV and hydrocortisone 200 mg IV and then restart the infusion at a slower rate.
- For more significant reactions, treat with adrenaline. See Anaphylaxis.
- The Australasian Consensus guidelines give specific advice in the event of late presentation, staggered overdose, therapeutic overdose and slow release preparations.
Topic Code: 2254