Send Feedback
Print
Mobile
Back
Poisoning / Drug Overdose
Management Priorities
Poisonings are a common cause of Emergency Department presentation. Roughly half involve intentional self-harm overdoses or recreational drug use in adults. The other group is children under 5 years with accidental exposure to medications, household chemicals or plants.
Poisoning is a major cause of death in patients under 40 years of age. However if a patient survives to reach hospital then the overall mortality is much less than 1%. This outcome is due mostly to good supportive care. Clinical advice can be obtained from Emergency Medicine staff or the National Poisons Centre (0800POISON). The approach to a poisoned patient can be summarized as follows:
- Resuscitation
- Risk assessment
- Supportive care and monitoring
- Investigations
- Decontamination
- Enhanced elimination
- Antidotes
- Disposition
Appropriate reference material and advice:
- The Toxicology Handbook 2nd edition (Murray, Daly, Little, Cadogan Churchill Livingstone, Sydney) - a concise and practical guide appropriate for Australasian practice.
- TOXINZ.com - an on-line reference available in the Emergency Department and Clinical Pharmacology Drug Information Service.
- Clinical Pharmacology Drug Information Service
 80900 or via the intranet.
80900 or via the intranet. - Emergency Medicine Physician, Clinical Pharmacologist or General Physician.
Telephone advice:
- URGENT: telephone 0800 POISON / 0800 764 766.
- Non-urgent: Monday to Friday 0900-1700 hours (03) 479 7227 and ask for Poisons Centre.
Resuscitation - Airway, Breathing, Circulation and Supportive Treatment
- The first priority in all unwell patients is attention to:
- Airway, Breathing, Circulation: See The ABCs
- Many poisoning patients have potential A, B and C problems which should be anticipated, identified, then managed expediently.
- Central nervous system depression or convulsions can cause problems with airway and breathing. Arrhythmias or cardiovascular depression are serious consequences of some poisonings.
- Seizures should be anticipated by the type of poison ingested. Common causes are tricyclic antidepressants, venlafaxine and amphetamines (including 'legal' recreational drugs). Most toxic seizures will respond to benzodiazepines in sufficient doses. Phenobarbitone is second line. Level of consciousness and airway must be closely monitored if using this agent. Phenytoin is contraindicated for toxic seizures.
- Check for hypoglycaemia, hypothermia or hyperthermia. A core temperature above 38.5ºC from a toxic cause is associated with serious toxicity and requires urgent cooling.
- The majority of poisoned patients can be managed supportively and expectantly. A few require gastrointestinal decontamination. This should not be considered routine but an intervention with specific indications. A small number of drugs have specific antidotes and these should be used judiciously.
Risk Assessment
The key step to managing poisoned patients is a realistic estimation of the likely toxicity expected for a poisoning episode. This prediction should include the maximum possible effect on the patient and the likely time course of events.
This assessment will provide a quick guide to whether the effects are likely to improve or worsen. Toxicity can be estimated as nontoxic, mild, moderate or severe. The pros and cons of possible interventions are balanced against this careful assessment of risk.
Key information:
- Identify the poison correctly (careful with trade names and homonyms).
- Estimate dose taken and express as per kg body weight. If unknown, estimate from the maximum amount that could have been taken.
- Time of exposure (is peak absorption expected soon or has it passed?).
- Clinical features already observed: signs and toxidromes.
- Refer to current poisons reference database or text.
- Consider the patient's intent in relation to the poison exposure. A serious suicide attempt is usually associated with large doses, whereas exploratory ingestions by small children are almost always sub toxic.
Toxidromes: a number of toxins/poisons produce recognisable toxic syndromes which may be rapidly identified at the bedside. These indicate systemic toxicity.
- Anticholinergic, e.g., tricyclics, antihistamines: Dry, warm skin; thirst and tachycardia; hyperthermia; confusion and hallucinations; urinary retention; visual disturbances.
- Sympathomimetics, e.g., amphetamines, cocaine, caffeine, theophylline: CNS excitation and convulsions; hypertension; tachycardia; sweating; mydriasis.
- Muscarinic, e.g., organophosphates, some mushrooms: Defecation, urination, miosis, bradycardia, emesis, lacrimation, salivation (DUMBELS).
- Nicotinic e.g., insecticides: Tachycardia, hypertension, muscle fasciculations, weakness, paralysis.
- Narcotic: CNS depression, hypotension, hypoventilation, miosis.
- Withdrawal e.g., from opioids, alcohol, benzodiazepines: Diarrhoea, mydriasis, tachycardia, lacrimation, abdominal pain, hallucinations, piloerection.
Supportive Care
Good supportive care of vital functions is probably the most important aspect of managing the poisoned patient.
A good management plan involves documenting:
- The type of observations required, noting the expected side effects of poisoning.
- Triggers for notification of medical staff.
- Criteria for changing management.
- Plan for psychosocial risk assessment where suicidal intent is suspected.
Investigations
Vital signs, blood glucose and ECG are important basic investigations.
A screening paracetamol level is advisable in self-harm poisonings. Paracetamol toxicity has no early clinical signs and fulminant hepatic toxicity is preventable if treatment is started early. A venous blood gas may detect acidosis or severe hypercapnia. Specific drug levels may be of use with a limited number of drugs:
- Carboxyhaemoglobin
- Carbamazepine
- Salicylate
- Digoxin
- Methanol
- Iron
- Lithium
- Valproic acid
Toxicology screening of urine is available but is rarely used to guide management.
A number of drugs can cause QT prolongation with the associated risk of torsades de pointes (TdP), e.g., haloperidol, chlorpromazine, citalopram, etc.
ECGs can be taken and the QT interval plotted on the nomogram below to assess the risk of TdP. The nomogram is more reliable than the QTc as the QTc underestimates the risk of TdP at low heart rates. A QT interval measured above the nomogram line should be considered a risk for TdP. These patients should have a period of cardiac monitoring or serial ECGs until the QT normalizes.
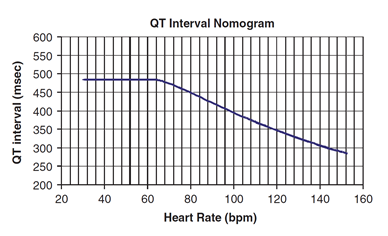
The QT nomogram is a risk assessment tool that accurately predicts arrhythmogenic risk for drug-induced QT prolongation. The sensitivity and specificity of the QT nomogram is 97% and 99% respectively (Bazett QTc =500 ms is 94% and 97% respectively).
Reference: Chan A, Isbister GK, Kirkpatrick CM, Dufful SB. Drug-induced QT prolongation and torsades de pointes: evaluation of a QT nomogram. QJM. 2007 Oct;100(10):609-15.
Decontamination of the Gastrointestinal Tract
After attention to ABC and risk assessment, gastrointestinal decontamination measures may be considered. There is no strong evidence that decontamination improves major outcomes. Decontamination is therefore not routine, but considered if significant toxicity is likely. The method chosen must have the potential to be effective with minimal risk to the patient.
The options include:
- Activated charcoal
- Gastric lavage
- Whole bowel irrigation
Activated Charcoal
- First choice for gastrointestinal decontamination, if any is indicated.
- Give 1 g/kg body weight (max 50 g) as a single dose orally.
- Repeated doses are indicated with some poisonings to interrupt the enterohepatic circulation and possibly as enteral dialysis (e.g., theophylline slow-release).
- The following substances are not adsorbed well to activated charcoal and therefore, alternative decontamination methods should be considered: ethanol, methanol, ethylene glycol, hydrocarbons such as petroleum distillates and essential oils, lithium, iron, potassium and lead (remember: alcohols, acids, alkalis, ions, metals).
- Charcoal should be given only if the perceived benefits outweigh the risks. Activated charcoal may cause vomiting, and if aspirated, will cause a lung injury. It should not be used for trivial or low risk overdoses. There are some overdoses where charcoal is effective greater than 1 hour after ingestion. Consult the TOXINZ internet database.
- Charcoal should not be given to patients who may become unconscious or have seizures (unless they are already intubated).
Gastric Lavage
- The indications for gastric lavage are very limited. Consider for a serious poisoning in which charcoal is ineffective and the airway is protected. Consult senior medical staff if you think it is indicated.
Whole Bowel Irrigation
- May be considered for serious poisonings with:
- Significant overdoses with sustained release preparations (e.g., theophylline, calcium channel blockers).
- Significant overdoses with substances not well bound by activated charcoal (e.g., iron, lithium, lead).
- Use polyethylene glycol (e.g., Klean-Prep™). Call the National Poisons Centre for the latest protocol.
There are many practical difficulties. Consultation with senior medical staff is essential.
Enhanced Elimination
These may include alkaline diuresis, haemodialysis or haemofiltration. Consult with senior medical staff. Haemoperfusion is not readily available at Christchurch Hospital.
Antidotes
- Logical antidotes antagonize at the level of cellular mechanisms, e.g., naloxone for narcotics and flumazenil for benzodiazepines, N-acetylcysteine for paracetamol.
- Empiric antidotes are drugs designed to achieve a physiological result, e.g., inotropes to restore blood pressure, atropine to raise heart rate etc.
- There are few specific antidotes that have proven benefit without significant risk of adverse effects. N-acetylcysteine is a good example. Other agents should be used judiciously.
Case Management
- Most patients will be assessed, observed, and discharged from ED.
- Patients who are critically unwell, unstable, or who require airway management or dialysis are admitted to ICU under a General Medicine Team.
- Patients who require prolonged antidotal treatment or who are expected to have prolonged toxicity (>12 hours) should be referred to General Medicine for admission.
- Those requiring prolonged cardiac monitoring who are alert and cooperative are admitted under General Medicine on telemetry (AMAU or Ward 12).
- Psychiatric Emergency Services are available if there is possible suicidal intent.
Topic Code: 1577