Send Feedback
Print
Mobile
Back
Spirometry
- Spirometry testing should be considered for all patients with symptoms or signs of lung disease such as cough, dyspnoea, wheezing, hyperinflation. This test can be useful to assess the severity of disease, progression of respiratory disease, or response to treatment.
- The first step for interpreting spirometry is to assess the FEV1/FVC ratio.
- If the ratio is less than the lower limit of the reference range (included with the test report), an obstructive defect is present.
- If the ratio is greater than the lower limit of normal, then spirometry is either normal or a restrictive defect may be present.
- The next step for interpretation is to assess the FVC.
- When the FVC is above the lower limit of normal, a restrictive pattern is excluded.
- When the FVC is below the lower limit of normal, a restrictive pattern is suggested which should be confirmed with total lung capacity (TLC) measurement.
- Spirometric restrictive patterns are correct only 50% of the time. Confirmation should be sought.
Once you diagnose obstructive lung disease on the FEV1/FVC pattern, the FEV1% predicted can be used to assess the severity of obstructive lung disease. The American Thoracic Society/European Respiratory Society (ATS/ERS) recommends the following severity classification in their 2005 standardization of lung function testing document.
|
|
Severity of any spirometric abnormality based on the forced expiratory volume in one second (FEV1), from ATS/ERS
|
Degree of severity
|
FEV1% predicted
|
Mild
|
>70
|
Moderate
|
60 - 69
|
Moderately severe
|
50 - 59
|
Severe
|
35 - 49
|
Very severe
|
<35
|
- Occasionally it might be useful to test for reversibility of airway obstruction after the administration of a bronchodilator. This test has a 90% specificity for the diagnosis of asthma, but only a 50% sensitivity (i.e., asthma can be missed by this test). ATS/ERS define an improvement in the FEV1 or FVC of 12% and at least 200 mL after bronchodilator administration as significant reversibility and asthma should be considered.
- Occasionally more complex lung function tests are useful to investigate a patient problem in detail. ATS/ERS suggest the following flow diagram in interpreting lung function testing. Prior to requesting these tests, they should be discussed with the respiratory physiology laboratory.
Interpretation of Lung Function Tests
Interpretation of Lung Function Tests
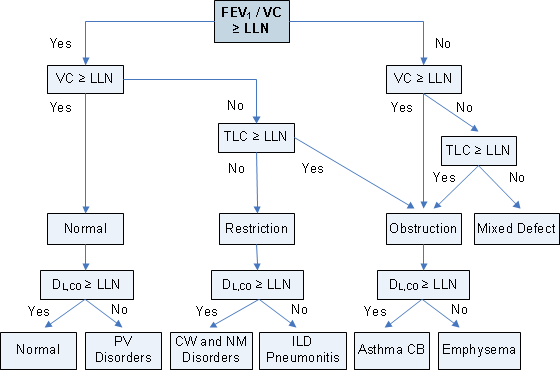
Reference: From ATS/ERS Pellegrino et al., 2005 Interpretative strategies for lung function tests. Eur Respir J 26, 948-968.
Note: LLN: lower limit of normal; PV: pulmonary vasculature; CW: chest wall; NM: neuromuscular; ILD: interstitial lung disease; CB: chronic bronchitis.
Topic Code: 3633